The future of medical coding is not manual: from ICD origins to auditable AI at scale
A tale as old as time
In 1837, a British statistician named William Farr faced a problem where every hospital used different names for the same diseases. His solution was to use one code per condition, a classification system that gave healthcare a common language for the very first time in history. A decade later, John Snow used that system to trace a cholera outbreak in London to a single contaminated water pump. That classification system became the original International Classification of Diseases, commonly abbreviated as ICD, where the original version had 161 codes.
Today, ICD-10-CM has over 70,000.
Medical coding is the backbone of how healthcare organizes payments, how population health pattens are understood, and how medical policies get established. Every diagnosis, procedure, and encounter needs to be translated into structured codes. Claims, research, and health policy all depend on that translation being accurate. When those translations aren’t, consequences like denied claims and compliance exposure exist.
For most of its history, that translation process has been a human job. The tools have evolved over time, but the underlying approach has not changed as much as the industry would like to believe.
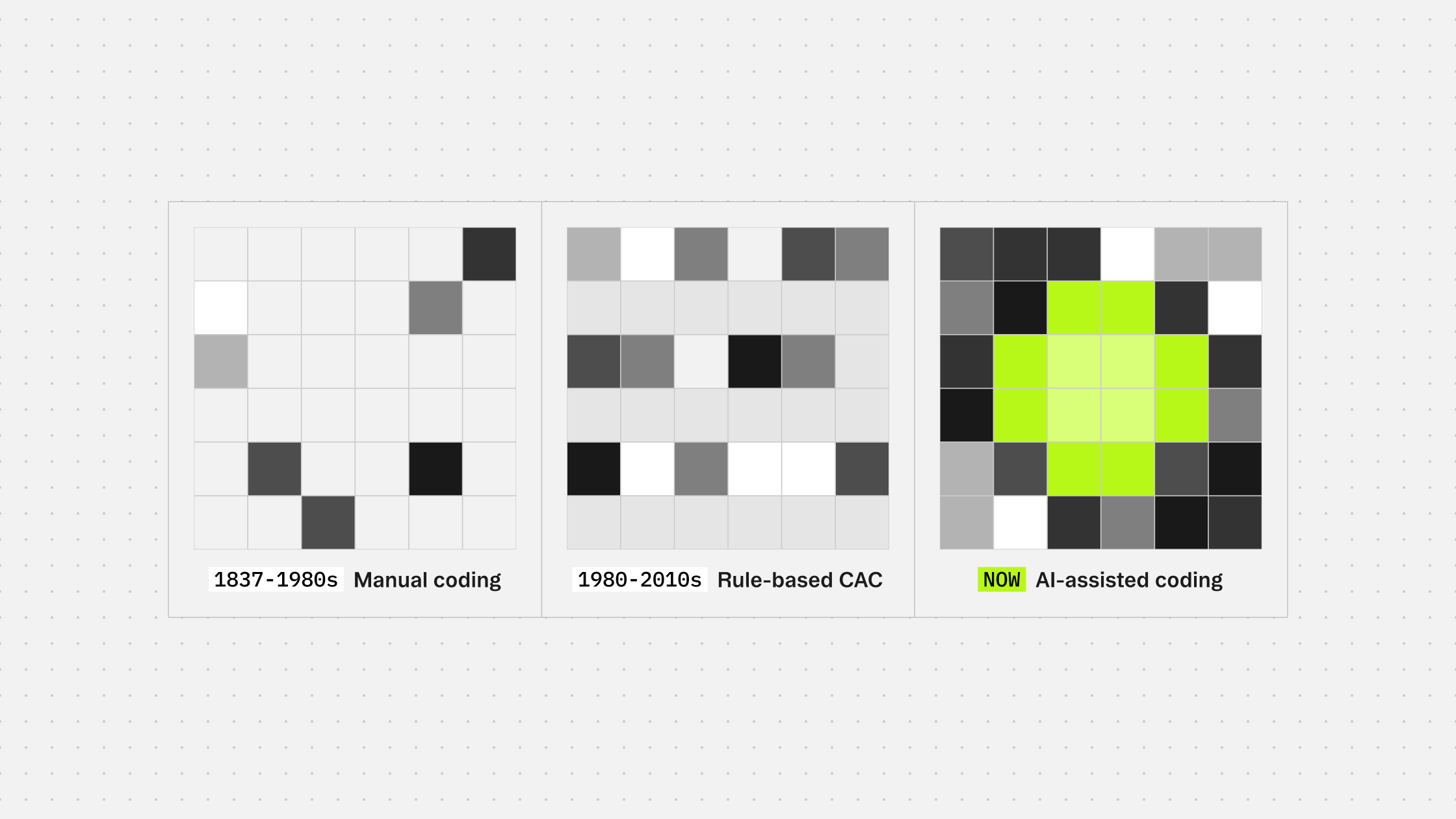
The evolution
Initially, trained coders read clinical notes, applied judgment drawn from thick rulebooks, and assigned codes, all manually and by hand. At smaller volumes, it worked and was effective. But as healthcare operations scaled, it became untenable fast.
The first wave of automation was rule-based. Computer-assisted coding tools worked essentially like a search function: match phrases in a clinical note against a predefined dictionary, surface the codes that fit. This was fast for common cases but quite slow for cases that came about once in a blue moon. These computer-assisted coding tools could not handle negations and context at the level of a human trained coder. And they still still cannot.
The next wave was machine learning. Models that trained on annotated clinical data could generalize beyond exact phrase matching and handle more complexity. Accuracy improved, but the approach introduced new issues. Models learned from whatever the training data contained, including its errors. They struggled with rare codes that appeared infrequently in training sets. They performed well on the hospitals whose data they were trained on and poorly everywhere else. And every year when ICD codes updated, the entire retraining cycle started again.
The reality of the workforce
According to the U.S. Bureau of Labor Statistics, employment of medical records specialists is projected to grow 7% from 2024 to 2034, with approximately 14,200 openings per year over that period.
With that being the case though, the coders who are in the workforce are feeling the squeeze. With fewer people coding higher chart volumes under the same turnaround expectations, accuracy has been suffering. In 2023, the AHIMA found that 66% of health information professionals reported understaffing in a recent workforce survey, with decreased reimbursement and slower claims processing as direct consequences. Three years later, understaffing is still an issue in the healthcare workforce, and hiring more coders is not a sustainable path forward.
So what does this all mean?
The question healthcare is starting to ask is a different one: what if coding were treated as an intelligence problem rather than a staffing one?
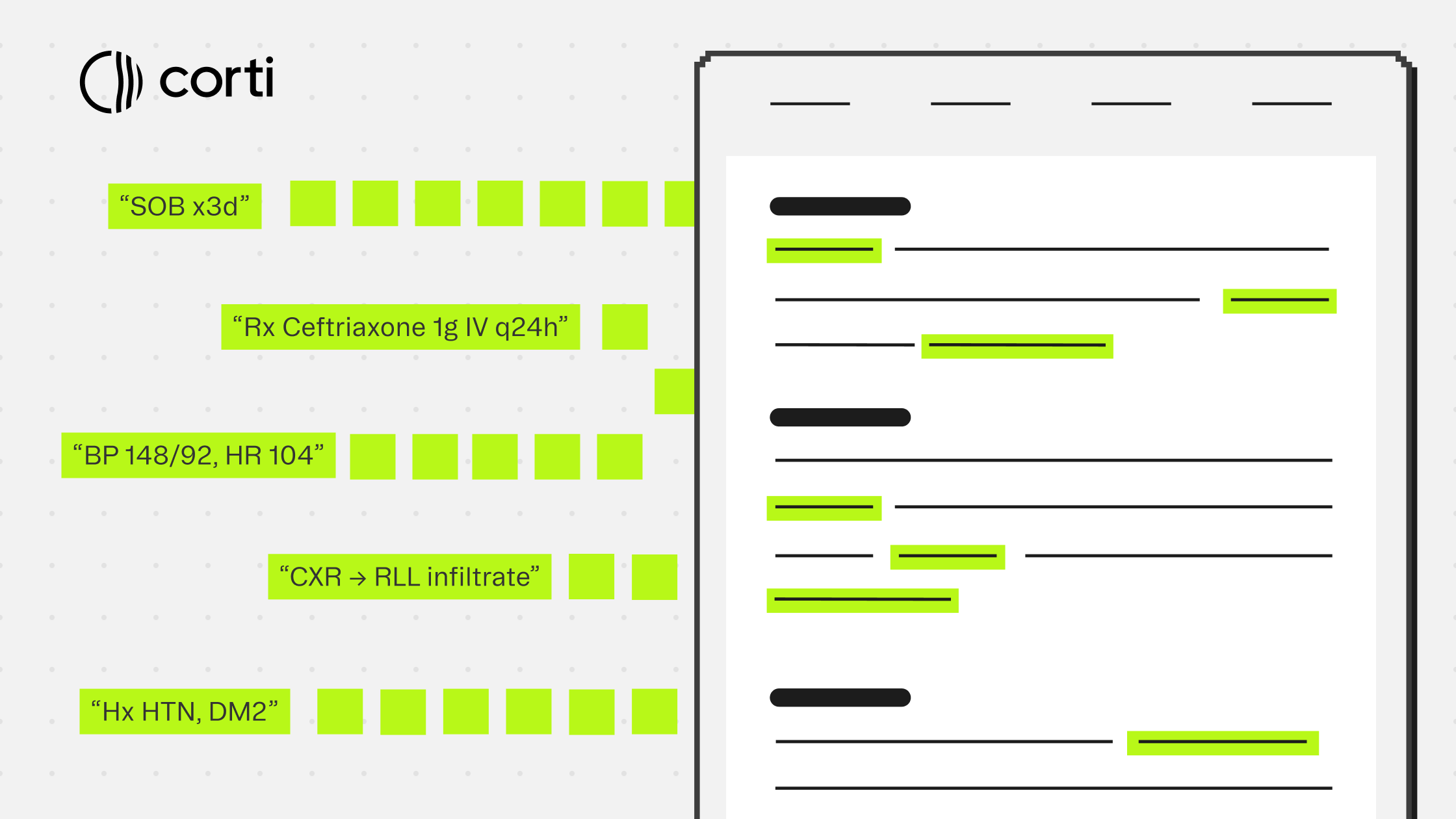
That framing changes what a solution looks like. Instead of tools that help coders do the same work faster, you need a system that can reason over clinical text the way a trained coder would. One that applies the rules of what should and should not be coded, selects the most specific appropriate code from the hierarchy, and returns output that is auditable at the prediction level.
That is the shift from human-first to AI-augmented. Human expertise does not disappear from this picture. It moves upstream, into review, exception handling, and the cases that genuinely require it. The volume work, the rules application, the evidence tracing: that is where AI earns its place.
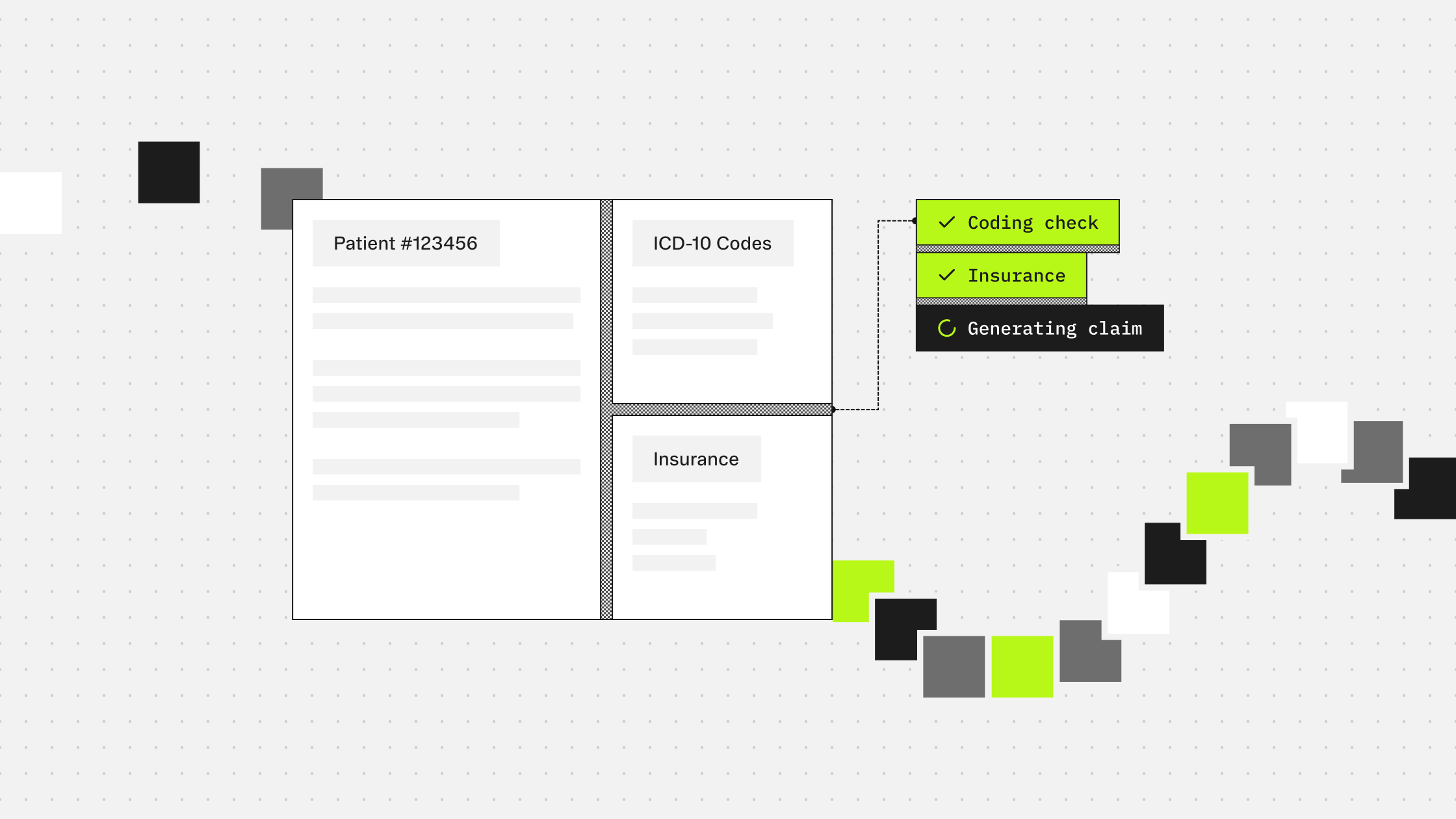
Corti has built Symphony for Medical Coding on exactly this premise. Rather than training a model on annotated coding data and inheriting the fragility that comes with it, the architecture encodes the logic of coding directly. What should be coded given the clinical context, what the guidelines say, and why.
This is early innings for AI-augmented coding. But the direction is clear. The organizations moving first are not replacing their coding teams. They are making them faster, more consistent, and harder to deny.
Next in this series: Where RCM breaks. A look at bottlenecks, leakage, and inefficiencies in current coding processes.
More guides to explore
Build faster. Ship safer. Scale smarter.
Get started with healthcare-native APIs built to power real clinical workflows.