AI-native RCM companies: who is building, where gaps remain, and why builders need APIs
A look at the landscape of companies building in the space
The revenue cycle management market has attracted a wave of AI-native companies over the past several years. Understanding who is building what, and where the gaps remain, matters if you are making decisions about what to build or buy.
Who is building in this space
The companies that have gained the most traction, Fathom, Nym Health, CodaMetrix, and Ambience Healthcare among them, share a common profile. They are purpose-built AI applications targeting health systems and RCM teams directly. They have real customers, real deployments, and real evidence that AI can improve on the legacy CAC and manual coding workflows they are replacing.
These are not marginal players. Fathom has processed tens of millions of charts. CodaMetrix has deep integration with major EHR systems. Nym has published peer-reviewed research on its approach. This is a well-funded, fast-moving category with genuine clinical credibility.
What they have in common
Most of these companies are built on one of two technical foundations. Some fine-tune large language models on annotated clinical data. Others combine traditional NLP with machine learning classifiers trained on historical coding records.
Both approaches have improved meaningfully on what came before. The accuracy numbers are real. The workflow integrations are real. Health systems have seen measurable reductions in denials and coder workload.
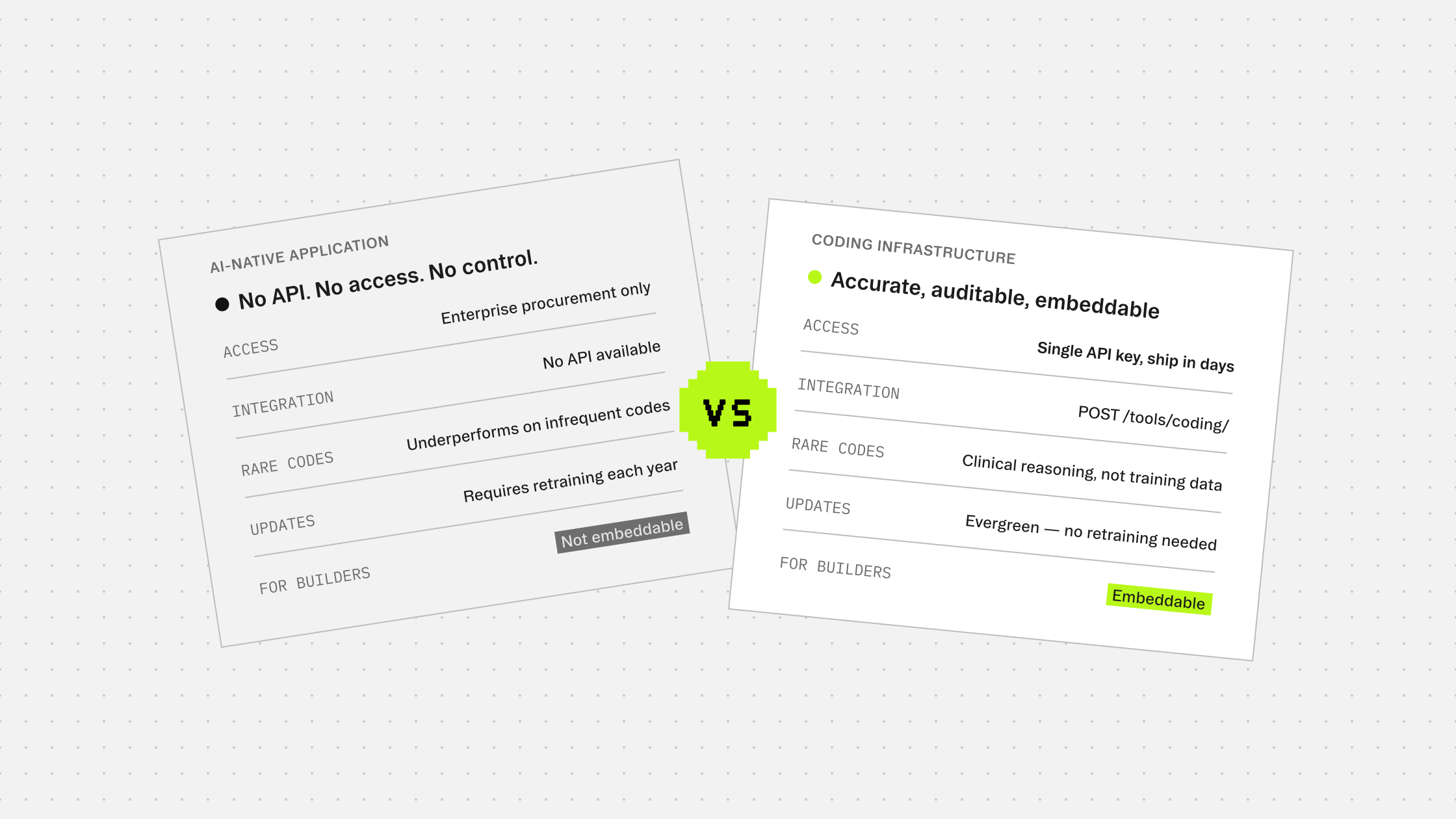
The limitation shared across both approaches is structural. When your model learns from annotated training data, it inherits the quality of that data. Rare codes that appear infrequently in training sets are systematically underperformed. A model trained on one hospital's records generalizes poorly to a different specialty mix elsewhere. And every October, when ICD codes update, the retraining cycle starts again. That is not a fixable bug. It is a property of how the models are built.
The infrastructure gap
There is a second thing most of these companies have in common: they are applications, not infrastructure.
They are sold to health systems through enterprise procurement cycles with implementation timelines measured in months. They sit inside a workflow rather than inside a product. For health systems evaluating a direct vendor relationship, that is exactly what they need.
For the growing category of builders, the EHR platforms, ambient documentation companies, and RCM point solutions that want to embed coding capabilities into their own products, those applications are the wrong shape. There is no clean API to drop into a workflow. Integration means either scraping outputs from a vendor UI, building a fragile workaround, or outsourcing charts to a coding service and waiting.
That gap is where infrastructure plays.
What this means for the market
The AI-native RCM companies are potential customers for coding infrastructure, not competitors to it. A company like Fathom or Ambience that has built a documentation or coding workflow on top of a fine-tuned LLM is exactly the kind of team that benefits from an API that handles coding accurately without requiring them to maintain a training pipeline or manage annual update cycles themselves.
The value proposition is different from a health system sale. It is about giving product teams a capability they can embed and ship, with accuracy that holds up on rare codes and edge cases, and output that is auditable at the prediction level so their end customers can trust it under payer scrutiny.
As the RCM automation market matures, the distinction between application and infrastructure will sharpen. Applications will consolidate around the workflows and buyer relationships where they have deepest traction. Infrastructure will move into the stack underneath, handling the parts of the problem, like accurate, evergreen, auditable coding, that every application in the category needs but none wants to maintain.
More guides to explore
Build faster. Ship safer. Scale smarter.
Get started with healthcare-native APIs built to power real clinical workflows.